Analytical characterization
Structural and functional characterization of molecular similarity5
PAVBLU® (aflibercept-ayyh) is indicated for the treatment of Neovascular (Wet) Age-Related Macular Degeneration (AMD), Macular
Edema following Retinal Vein Occlusion (RVO), Diabetic Macular Edema (DME), and Diabetic Retinopathy (DR).
PAVBLU® is not indicated for Retinopathy of Prematurity, for which Regeneron has marketing exclusivity.
PAVBLU® (aflibercept-ayyh) is indicated for the treatment of Neovascular (Wet) Age-Related Macular Degeneration...Read more
PAVBLU® (aflibercept-ayyh) is indicated for the treatment of Neovascular (Wet) Age-Related Macular Degeneration (AMD), Macular
Edema following Retinal Vein Occlusion (RVO), Diabetic Macular Edema (DME), and Diabetic Retinopathy (DR)...Read more

| FDA Requirements for Biosimilar Approval | Totality of Evidence for PAVBLU® |
|---|---|
Analytical characterizationStructural and functional characterization of molecular similarity5 |
Comparative analytical similarity assessments demonstrated that PAVBLU® and EYLEA® have the same amino acid sequence and exhibit similar higher-order structure and biological activity.3 |
Nonclinical studiesDemonstrating similar mechanism of action, potency, immunogenicity, and toxicity5 |
Nonclinical assessments of pharmacology, pharmacokinetics, toxicokinetics, and safety for PAVBLU® were conducted to support similarity to EYLEA®.4 |
Clinical pharmacologyConfirming biosimilarity with pharmacokinetics and pharmacodynamics5 |
Results from a clinical pharmacology substudy demonstrated pharmacokinetic similarity between PAVBLU® and EYLEA®.2 |
Comparative clinical studyProving no clinically meaningful differences in safety, efficacy, or immunogenicity in a sensitive patient population5,* |
A randomized comparative clinical study in 576 subjects with neovascular (wet) age-related macular degeneration (AMD) demonstrated no clinically meaningful differences in efficacy, safety, and immunogenicity between PAVBLU® and EYLEA®.2 |
|
|
Single-transition studyIn the clinical study, half of patients in the EYLEA® arm were rerandomized to receive PAVBLU®. Results showed no clinically meaningful differences following transition.2 |
*Adequately sensitive to detect clinically meaningful differences between the reference product and the proposed biosimilar, should they exist.


*Neovascular (wet) AMD in the study eye with active treatment-naïve subfoveal CNV lesions secondary to neovascular (wet) AMD, including juxtafoveal lesions that affect the fovea as confirmed with SD OCT, FA, and/or FP in the study eye.
BCVA = best corrected visual acuity; CNV = choroidal neovascularization; CST = central subfield thickness; ETDRS = Early Treatment Diabetic Retinopathy Study; FA = fluorescein angiography; FP = fundus photography; IVT = intravitreal; SD OCT = spectral domain optical coherence tomography.
Patient characteristics were balanced between treatment arms
|
Selected Baseline Patient Characteristics (mean) |
PAVBLU® (n = 288) | EYLEA® (n = 288) |
|---|---|---|
| Age, years | 76.0 | 76.0 |
| Duration of disease, weeks | 7.4 | 6.7 |
| BCVA ETDRS letter score | 58.9 | 57.6 |
| CNV area size, mm2 | 8.5 | 9.3 |
| CST, µm | 438.4 | 448.8 |
BCVA = best corrected visual acuity; CNV = choroidal neovascularization; CST = central subfield thickness; ETDRS = Early Treatment Diabetic Retinopathy Study.



Proportion of subjects who maintained vision at week 52 (lost < 15 letters in ETDRS letter score compared with baseline)
Proportion of subjects who gained ≥ 10 letters of vision at week 8 (ETDRS letter score)
Proportion of subjects who gained ≥ 15 letters of vision at week 52 (ETDRS letter score)
*Estimated using ANCOVA model adjusted for the stratification factors, geographic region (East Asia, Europe, North America), and baseline BCVA as covariates.
BCVA (ETDRS letter score) data values provided for select endpoints: PAVBLU® (n = 273) mean change from baseline (59) at week 8 (+6.5) and week 52 (+7.6); EYLEA® / PAVBLU® (n = 134) mean change from baseline (57.8) at week 8 (+5.6) and week 52 (+8.0); EYLEA® (n = 136) mean change from baseline (57.2) at week 8 (+7.6) and week 52 (+9.4).
†Half of patients in the EYLEA® arm were rerandomized to receive PAVBLU® at week 16 and the first assessment after rerandomization occurred at week 24. Patients who discontinued prior to the first assessment after rerandomization were not included in this secondary endpoint analysis.


CST data values provided for select endpoints: PAVBLU® (n = 273) mean change from baseline (439.4) at week 8 (-145.9) and week 52 (-157.1); EYLEA® / PAVBLU® (n = 134) mean change from baseline (458.8) at week 8 (-167.4) and week 52 (-177.4); EYLEA® (n = 136) mean change from baseline (440.3) at week 8 (-146.3) and week 52 (-159.1).
CNV area size data values provided for select endpoints: PAVBLU® (n = 273) mean change from baseline (8.6) at week 8 (-5.0) and week 52 (-6.3); EYLEA® / PAVBLU® (n = 134) mean change from baseline (9.2) at week 8 (-5.2) and week 52 (-6.4); EYLEA® (n = 136) mean change from baseline (9.5) at week 8 (-5.5) and week 52 (-7.3).
†Half of patients in the EYLEA® arm were rerandomized to receive PAVBLU® at week 16 and the first assessment after rerandomization occurred at week 24. Patients who discontinued prior to the first assessment after rerandomization were not included in this secondary endpoint analysis.
‡Measured by spectral domain optical coherence tomography.
§Measured by fluorescein angiography.
ANCOVA = analysis of covariance; BCVA = best corrected visual acuity; CI = confidence interval; CNV = choroidal neovascularization; CST = central subfield thickness; ETDRS = Early Treatment Diabetic Retinopathy Study.
You can expect PAVBLU® to provide highly similar therapeutic benefits to EYLEA® for your patients
| Most common treatment-emergent adverse events (≥ 1%) THROUGH week 16 | ||
|---|---|---|
| Treatment-Emergent Adverse Events* | PAVBLU® (n = 288)% (n) | EYLEA® (n = 288)% (n) |
| Conjunctival hemorrhage | 4.2% (12) | 3.8% (11) |
| Injection site pain | 1.4% (4) | 0.3% (1) |
| Conjunctival hyperemia | 1.0% (3) | 0.0% (0) |
| Intraocular injection complication | 1.0% (3) | 0.0% (0) |
| Posterior capsule opacification | 1.0% (3) | 1.0% (3) |
| Retinal hemorrhage | 0.7% (2) | 1.4% (4) |
| Retinal pigment epithelial tear | 0.3% (1) | 1.4% (4) |
| Visual acuity reduced | 0.3% (1) | 1.4% (4) |
| Dry eye | 0.0% (0) | 1.4% (4) |
| Vitreous detachment | 0.0% (0) | 1.0% (3) |
| Vitreous floaters | 0.0% (0) | 1.0% (3) |
| Most common treatment-emergent adverse events (≥ 1%) Post Week-16 rerandomization THROUGH WEEK 52 | |||
|---|---|---|---|
| Treatment-Emergent Adverse Events* | PAVBLU® (n = 273)% (n) | Eylea®/PAVBLU® Eylea® / PAVBLU® (n = 133)% (n) | Eylea® (n = 136)% (n) |
| Visual acuity reduced | 2.9% (8) | 3.8% (5) | 0.7% (1) |
| Cataract | 2.2% (6) | 0.8% (1) | 2.2% (3) |
| Retinal hemorrhage | 1.8% (5) | 3.0% (4) | 0.7% (1) |
| Chalazion | 1.1% (3) | 0.0% (0) | 0.0% (0) |
| Conjunctival hemorrhage | 1.1% (3) | 6.0% (8) | 3.7% (5) |
| Macular fibrosis | 1.1% (3) | 0.0% (0) | 0.7% (1) |
| Subretinal fluid | 1.1% (3) | 0.8% (1) | 0.0% (0) |
| Vitreous detachment | 1.1% (3) | 0.8% (1) | 0.0% (0) |
| Posterior Capsule Opacification | 0.7% (2) | 0.8% (1) | 2.2% (3) |
| Visual Impairment | 0.7% (2) | 0.8% (1) | 1.5% (2) |
| Vitreous floaters | 0.7% (2) | 1.5% (2) | 1.5% (2) |
| Macular edema | 0.4% (1) | 1.5% (2) | 0.7% (1) |
| Ocular hypertension | 0.4% (1) | 1.5% (2) | 0.0% (0) |
| Ocular hyperemia | 0.0% (0) | 0.0% (0) | 1.5% (2) |
| Injection site pain | 1.1% (3) | 0.8% (1) | 0.0% (0) |
| Sensation of foreign body | 0.4% (1) | 0.8% (1) | 1.5% (2) |
Note: Only treatment-emergent adverse events were summarized. For each adverse event of interest, subjects were included only once, even if they experienced multiple events for that adverse event of interest.
*Adverse event of interest identified using MedDRA v25.1 terms.
†Adverse events of interest (EOI) prespecified for this study were endophthalmitis, retinal detachment, increase in intraocular pressure, and thromboembolic events.
Comparable safety profile was demonstrated across
all treatment groups, including patients who transitioned
from EYLEA® to PAVBLU®
Study design: A retrospective, observational study of 1,000 eyes treated with PAVBLU® using electronic medical records (EMRs) from retina practices in the United States to describe demographics, utilization, visual outcomes (best recorded visual acuity), and safety analysis (adverse events of special interest) among 989 adult patients diagnosed with nAMD, RVO, DME, or DR. Records from December 1, 2024, to October 31, 2025, were included in this interim analysis, focusing on eyes with ≥ 84 days of follow-up. Bilaterally treated eyes from the same patient were included and analyzed as independent study eyes. Data were extracted from EMRs of patients seen by 175 retina specialists at 146 locations across 24 states using Structured Query Language (SQL). The index date was defined for each eye as the date of the first documented PAVBLU® injection.
Important considerations: This descriptive study was not designed to compare PAVBLU® with other anti-VEGF therapies, there was no concurrent comparator arm, and patients were not randomized. The planned primary assessment timepoint of ~ 3 months limits conclusions on longer-term visual outcomes, durability, and rare adverse events. Analysis of the full 12-month follow-up period is pending.
| Patient Population |
|---|
| 989 patients with nAMD, RVO, DME, DR |
| 1,000 consecutively treated eyes |
| 3,730 intravitreal injections of PAVBLU® |
| ≥ 84 days follow-up from first injection |
| Disease Distribution (n = eyes) | ||
|---|---|---|
| Neovascular (wet) age-related macular degeneration (nAMD) | (n = 578) | 58% |
| Macular edema following retinal vein occlusion (RVO) | (n = 193) | 19% |
| Diabetic macular edema (DME) | (n = 162) | 16% |
| Diabetic retinopathy (DR) | (n = 67) | 7% |
| 91% of eyes (n = 906) transitioned from prior therapy |
|---|
| Median number of prior anti-VEGF injections = 21 (8-46 IQR range) |
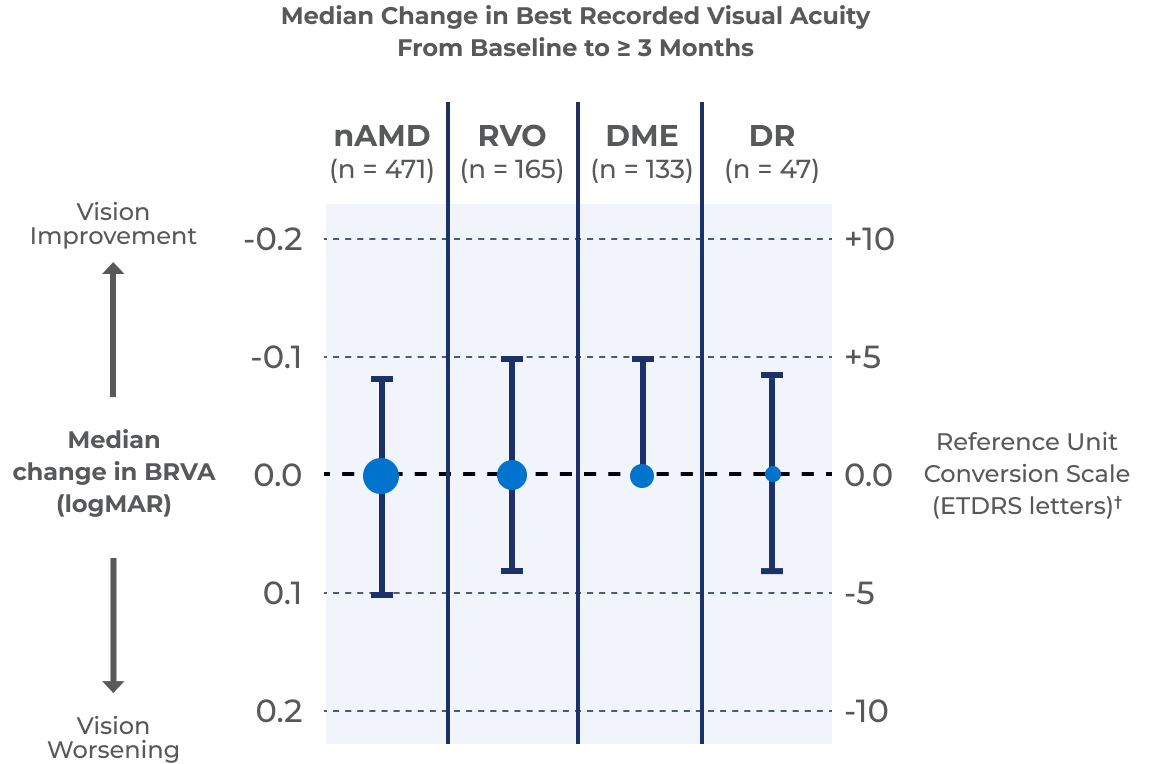
| Best Recorded Visual Acuity (mean) |
| Baseline: 0.4 logMAR (~ 20/50)† |
| ≥ 3 Months: 0.4 logMAR (~ 20/50)† |

| 9% of eyes (n = 94) were anti-VEGF treatment-naïve |
|---|
| Small sample sizes in subgroups limit interpretability |
| Best Recorded Visual Acuity (mean) |
| Baseline: 0.5 logMAR (~ 20/63)† |
| ≥ 3 Months: 0.4 logMAR (~ 20/50)† |
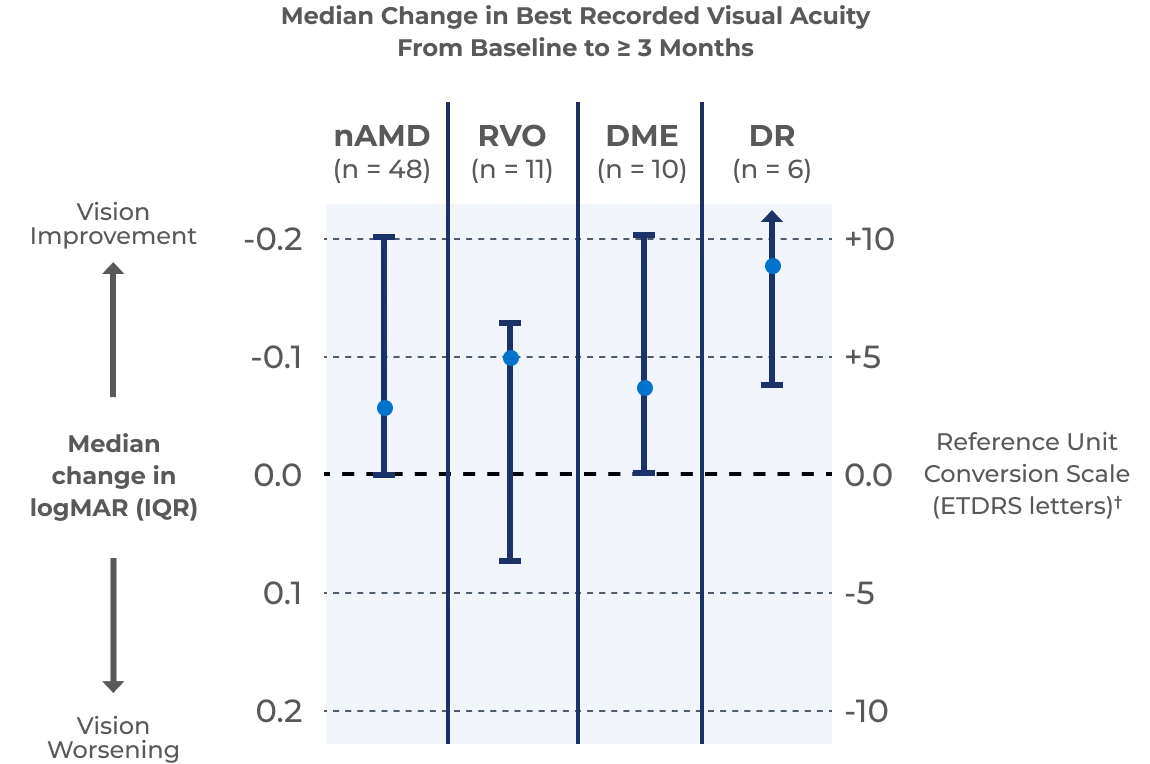

*Analyses of best recorded visual acuity (BRVA) outcomes focused on eyes with at least 84 days of follow-up after the index date. BRVA, recorded as Snellen visual acuity and converted to logMAR for analysis, was assessed at baseline and at ≥ 84 days of follow-up. Continuous variables were summarized using means and standard deviations or medians and interquartile ranges (IQRs), as appropriate.
†Visual acuity unit conversion logMAR to Snellen (feet) and ETDRS letters.2
Defined AESIs were endophthalmitis, retinal vasculitis, iritis, vitreous cells, retinal detachment, and vitreous hemorrhage. The number of injections in the study is insufficient to estimate the rate of these adverse events of special interest.‡
‡Adverse events of special interest (AESIs), defined as adverse events occurring within 21 days of any PAVBLU® treatment, were identified in EMRs according to clinical and imaging findings and supported by ICD-10 codes, with manual chart reviews performed by investigating physicians to validate extracted data. Both cases of iritis resolved with topical steroid treatment.
An investigator-led, observational analysis of a large safety dataset provides an assessment of real-world safety outcomes from 11,529 patients treated with PAVBLU® (aflibercept-ayyh) 2 mg intravitreal injections. The data from 15,143 eyes (including 4,070 eyes with > 6 months of follow-up) were collected from 4 retina centers in the United States and identified through manual and keyword search from a large database.
The APEX real-world safety analysis of 52,374 PAVBLU® injections reported no new safety findings in this dataset; ocular adverse events reported included ocular hypertension, endophthalmitis, intraocular inflammation, retinal vasculitis, and retinal vascular occlusion.
Important Considerations: The data were aggregated at the injection level rather than patient level, meaning the severity, management, and clinical outcomes of ocular events could not be evaluated in detail. This descriptive study was not designed to compare PAVBLU® with other anti-VEGF therapies, there was no concurrent comparator arm, and patients were not randomized. The reported cases of endophthalmitis were considered injection-related ocular adverse events, rather than drug-attributable adverse reactions.
These real-world data provide initial insight into the use of PAVBLU® in routine clinical practice
You are encouraged to report negative side effects of prescription drugs to the FDA.
Visit www.fda.gov/medwatch, or call 1-800-FDA-1088.
PAVBLU® (aflibercept-ayyh) is indicated for the treatment of Neovascular (Wet) Age-Related Macular Degeneration (AMD),
Macular Edema following Retinal Vein Occlusion (RVO), Diabetic Macular Edema (DME), and Diabetic Retinopathy (DR).
PAVBLU® is not indicated for Retinopathy of Prematurity, for which Regeneron has marketing exclusivity.


